This patient was referred to Dr. Morganroth, a fellowship-trained and double board certified Mohs surgeon, for a large basal cell carcinoma of the nasal tip. Following Mohs surgery, the defect was quite extensive and was the result of delay in diagnosis. The early diagnosis of skin cancer results in a smaller skin defect and smaller scar. In patients with a history of skin cancer and those with an increased risk of skin cancer, twice-yearly full body skin checks are recommended.
This defect was quite large and the patient is a young professional who interfaced with clients every day. Dr. Morganroth reviewed the limited treatment options. For the best result historically for a defect that involves the entire nasal tip and extends into surrounding cosmetic units, the paramedian forehead is a very common approach. The paramedian forehead flap is a two or more stage procedure. Stage one is transferring skin from the forehead to the nose while the base of the forehead skin is still attached to the medial eyebrow where the skin gets its blood supply from an artery. The flap looks like an elephant trunk and extends from the medial eyebrow to the nasal tip. The artery provides nutrients to the flap similar to an umbilical cord while the forehead skin attached to the nasal defect develops its own blood supply. After three weeks, the forehead skin attached to the nasal tip has developed its own blood supply and the trunk or umbilical cord is no longer needed. The trunk is divided and the medial eyebrow and tip of nose sections are sutured into place in a second procedure.
The paramedian forehead flap is considered one of the most advanced reconstruction techniques and there are a limited number of Mohs surgeons who routinely perform this procedure. In many communities, these defects are sent to facial plastic, head and neck or plastic surgeons for the reconstruction in a 2 to 4 hour surgery under general anesthesia. Dr. Morganroth performs this procedure under local anesthesia in less than 30 minutes and has performed it countless times. Cases 11 and 12 are examples of the outcome of paramedian forehead flaps performed by our reconstructive surgeon Dr. Morganroth.
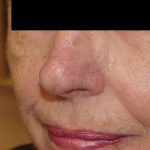
This patient declined the paramedian forehead flap because she did not want to have a multi-staged procedure over three weeks with a skin pedicle sutured to her nose. Dr. Morganroth felt the forehead flap would give a superior result to a full thickness skin graft and the size and location of the defect was at the upper limits for a successful local flap. Dr. Morganroth repaired this large defect completely under local anesthesia with a bilobed transposition flap. This repair provided a superior outcome versus the paramedian forehead flap since the local flap used the skin with the same color, texture and thickness. The local flap was also completed in one surgery, did not have a forehead scar (had a forehead flap been performed) and sutures were removed in 7 days allowing this professional to interface with clients in one week.