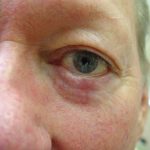
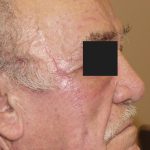
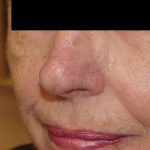
This patient presented with an ill-defined, recurrent nodular basal cell carcinoma on the nasal bridge that had been treated with topical 5-fluorouracil (Efudex) by her dermatologist to avoid surgery and a scar. Not unexpectedly, the topical chemotherapy agent failed to cure the nodular basal cell carcinoma. The cure rate for topical treatment of this type of skin cancer and location is known to be unacceptably low. Recurrent skin cancers on the face are absolute indications for Mohs surgery. Dr. Morganroth, a double-board certified Mohs surgeon performed Mohs surgery resulting in a large defect. The size of the defect was exacerbated by the prior treatment failure. Had Mohs surgery been done instead of the topical therapy, the tumor would have been treated earlier with a smaller resultant defect. Despite the large defect size, Dr. Morganroth used an adjacent tissue transfer or flap to mobilize adjacent skin of the same thickness, color and texture to obtain a nice result. The fine scars are the result of Dr. Morganroth’s multi-layered suturing technique consisting of two layers. The first layer consists of dissolvable sutures placed in the dermis where they are not visible to the patient and dissolve over a period of weeks to months. The second layer consists of fine sutures that are visible to the patient or cyanoacrylate glue to align the skin edges and provide support to the wound. The key to Dr. Morganroth’s nice scar results is his buried suture technique developed over tens of thousands of skin reconstructions, excisions, and scar revisions where routinely realigns the skin edges without the need for top sutures. All of the wound tension is supported by the bottom sutures that dissolve over weeks to months to allow the wound to heal completely. In contrast, many surgeons require both bottom sutures and the top sutures to completely close the wound. The bottom sutures are placed but do realign the skin edges leaving a gap. Additional top sutures are then required to get complete closure. Since the top sutures are under tension due to the pressure needed to close the skin edges completely, when the wound stretches overtime, the top sutures leave scars that look like “railroad tracks”. “Railroad track” scars are less likely when all of the wound tension is supported by the deep stitches beneath the skin surface. When the scar stretches as part of the normal healing, the deep sutures do not leave any stitch marks.