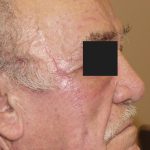
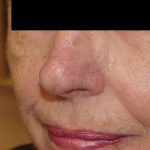
This patient presented with a non-healing, pearly bump on his nostril that had been treated one year earlier with cryosurgery by his primary care doctor. He sought Dr. Morganroth’s opinion as a fellowship-trained and double board certified Mohs surgeon. Dr. Morganroth performed a biopsy that revealed an infiltrative basal cell carcinoma. The infiltrative subtype is more aggressive and can be larger and deeper than non-aggressive basal cell carcinomas. Since this tumor had aggressive histology, had prior treatment with liquid nitrogen, and was located in a cosmetically sensitive area, Dr. Morganroth discussed the importance of treatment with Mohs surgery to obtain the highest possible cure rate and minimize the removal of normal skin. This cancer was removed in two stages of Mohs surgery resulting a the smallest possible defect size (with a cure rate of 99%) on the medial portion of the nostril cosmetic unit (the nostril defined by the nostril crease and rim). The challenges of this defect include the size, the central face location without any tissue movement (versus the cheek that has loose skin), and a location near the free margin of the nostril, and a location that could impact the nasal valve that can be pinched or altered under tension to decrease nasal airflow and negatively impact breathing.
The reconstruction options discussed with the patient included: allowing the defect to heal on its own; a linear closure; full thickness skin graft; and adjacent tissue transfer or flap.
Granulation or allowing the wound to heal by itself is a viable option but would take weeks to heal, may cause an upward retraction of the nostril margin as the wound contracts, and has an uncertain scarring outcome ranging from very good to problematic. A linear closure was not practical because pulling the skin edges together side-to-side without any adjacent loose skin would cause nostril distortion and asymmetry. A full thickness skin graft would be one the most common approaches to repair this defect because a skin graft would not cause any tension on the nostril and the nose shape and function would be unchanged. A full thickness skin graft procedure involves removing skin from another area of the face (ie. the ear or nasolabial fold), thinning the skin and then suturing it into the defect. The graft develops a blood supply from the base of the defect and heals to form new skin. The grafts can give a very good result but may leave a depression or thickened area with skin that has a different color or texture than the untreated adjacent skin. A flap is an advanced procedure commonly used by Mohs surgeons to repair defects in areas where the adjacent skin is tight and a linear closure is not practical. Flaps involve a number of mechanics to rearrange the adjacent skin including rotation of skin, advancement of skin, and transposition of skin to fill the defect with skin of the same color, thickness, and texture. Flap selection is critical to obtain the best possible result.
This defect is particularly challenging due to the location on the nostril where there is very little adjacent skin and no tissue that is loose or mobile. Mobilizing skin to fill this defect often extends the reconstruction area outside of the nostril cosmetic unit and may negatively impact the shape of the delicate nostril crease the defines the border between the nostril and nasal sidewall.
When Dr. Morganroth first began his practice, he was disappointed in the cosmetic results that he saw from full thickness skin grafts on the nostril performed by others in the community. He also was not happy with the most common flap outcome (using a transposition flap) because this flap blunted the delicate nostril crease creating obvious distortion. In his quest of find a better solution for a nostril defect, Dr. Morganroth developed a new flap technique 29 years ago that solved the problems with grafts (mismatched skin color, thickness and color) and transposition flaps (blunting of the nostril crease) by creating a flap that mobilized skin that was contained completely within the nostril cosmetic unit. By mobilizing skin entirely within the cosmetic unit, his repair used the same skin (color, thickness, texture) without impacting the nostril crease for a more consistent superior result. After performing a number of these procedures on his patients referred by other Silicon Valley dermatologists, he received very positive feedback from his patients and referring physicians. Dr. Morganroth recalls a phone call from dermatologist Georgia Abrams, MD in Saratoga who called him within a few years of his practice opening to report that his nostril reconstruction results were the best she had seen and she was going to refer all of her future skin cancer patients to him for surgery. Dr. Morganroth credits the innovation of this flap as the single most important event to impact the trajectory of his 30-year-old Mohs practice. Dr. Abrams later sold her practice to Dr. Morganroth and worked for him for many years until her retirement.
Cases 1, 2 and 3 are examples of Dr. Morganroth’s innovative flap and remains his treatment of choice to consistently obtain his best cosmetic result for defects in the nostril cosmetic unit. While this flap is a great option, patients with sebaceous skin (skin that is thickened by enlarged sebaceous glands and dilated pores) have higher rates of complications and may benefit from full thickness skin grafts harvested from ear skin sites that have a matching skin texture to the nostril site.