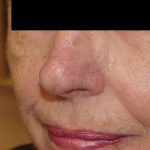
Lip skin cancers (and nasal and eyelid skin tumor) are one of the highest drivers of anxiety and concern for patients due to the uncertainty of cosmetic and functional outcomes. Dr. Morganroth specializes in reconstruction of the lips (and noses and eyelids) with the singular goal of producing the best possible cosmetic and functional outcomes using his broad reconstruction repertoire. This patient was self-referred based on her research after her dermatologist suggested topical chemotherapy to minimize the risk of a poor cosmetic outcome. Fortunately, the patient researched that topical chemotherapy has an unacceptably low cure rate for an infiltrative basal cell carcinoma on the lip. Dr. Morganroth, a double board-certified Mohs surgeon, performed Mohs surgery to obtain the highest possible cure rate and minimal sacrifice of normal skin. This defect was complicated in that it involved both the cutaneous lip and mucosal lip and ablated the vermilion border (fine line that defines the junction of the cutaneous lip and pink mucosal lip). This defect is challenging and is managed differently based on the individual surgeon’s personal preferences and experience. Some surgeons will excision the entire thickness of the lip in a wedge or “pie” shape to close this defect in a straight line. Dr. Morganroth finds this repair problematic for a number of reasons. First, there is an excessive removal of lip skin, muscle and mucosa resulting in the loss of alto of normal tissue. The scar if often hard to hide and there is transaction of the nerves and major blood vessels of the lip increasing the risk of complications. Lastly, the lip is shortened since a full thickness wedge permanently removes a percentage of the lip. Dr. Morganroth views this defect as a three area repair : 1. mucosal lip; 2. cutaneous lip; and 3. vermillion border. Dr. Morganroth’s approach preserves as much normal lip tissue as possible and keeps the incision and repair scars camouflaged. In this case, Dr. Morganroth made an incision along the vermilion border lateral to the defect and advanced the lip skin medially to repair the cutaneous lip using the natural vermillion border as the inferior aspect of the lip. The mucosa located inferior to the defect was advanced superiorly and sutured to the newly created vermillion border to recreate the mucosal lip cosmetic unit without adding any additional scarring. The outcome created a natural outcome without any distortion or the lip nor removal of lip muscle. One month post-op the results are excellent and the faint pink scar will resolve the next few months healing well within the expected one year healing period for a reconstruction scar.