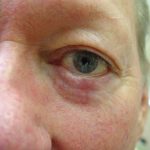
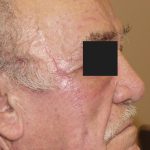
This patient had a morpheaform basal cell carcinoma which is an aggressive type of basal cell carcinoma that is much larger than what is visible with the naked eye. The patient’s primary concern was the impact of this skin cancer on his eyebrow and whether his eyebrow would be distorted after surgery. He was first seen by a plastic surgeon who recommended excision with frozen sections in a surgery center followed by a reconstruction that would involve reconstruction the eyebrow. He was informed that he would have a scar in the eyebrow but the eyebrow would be aligned and would make the scar (and interruption of eyebrow hair by the scar) less obvious. The patient sought a second opinion by Dr. Morganroth who recommended a different approach. First, Mohs surgery would offer the highest cure rate and remove the most minimal amount of normal skin. This high cure rate with the smallest possible scar would be the best chance of minimizing damage to the eyebrow. Second, Mohs surgery has a much higher cure rate for morpheaform basal cell carcinoma because 100% of the margin is evaluated histologically versus less than 1% of the margin for frozen excision in the surgery center. Third, Mohs surgery allows for smaller margins of excision to preserve as much skin as possible with the hope of sparing the eyebrow. Fourth, Mohs surgery is performed with local anesthesia and does not require a surgery center.
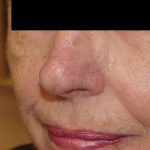
Following the completion of Mohs surgery with the expected 99% cure rate and minimal sacrifice of normal skin, the defect was large but did not enter the cosmetic unit of the eyebrow. Mohs surgery allowed a smaller excision margin and spared damage to the eyebrow. The next step was reconstruction of the defect in a manner that creates the best cosmetic outcome. Closing the defect in a horizontal linear closure would create an asymmetrical elevation of the brow that would be cosmetically unacceptable. A vertical linear closure would leave scar that would interrupt the continuity of the eyebrow and cause distortion to the upper lid skin. Dr. Morganroth chose to execute an advancement flap where the reconstruction surgery did not involve the cosmetic unit of the eyebrow. This reconstruction created minimal scarring without any distortion of the eyebrow.