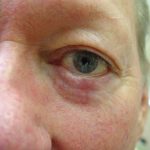
This patient had a nodular basal cell carcinoma on the lower eyelid and was referred to Dr. Morganroth, a double board-certified, fellowship-trained Mohs surgeon with tens of thousands of successful reconstructions. While any fellowship-trained Mohs surgeon can successfully remove an eyelid skin cancer, a much smaller percentage of Mohs surgeons are comfortable repairing eyelid defects due to the risk of eyelid retraction or droop from the reconstruction. Often these patients are referred to ophthalmic plastic surgeons to repair the Mohs defect. Dr. Morganroth can repair the majority of eyelid defects and occasionally sends large and complicated defects to ophthalmic plastic surgeons for specialized reconstruction that requires sedation.
Dr. Morganroth performed Mohs surgery to provide the highest cure rate and minimal sacrifice of normal skin. It was crucial to preserve the normal eyelid skin because a few extra millimeters of skin removal can dramatically impact the reconstruction options and outcome. This defect was repaired with a combination of a bilateral advancement flap and a full thickness skin graft with local anesthesia alone. The full thickness skin graft was harvested from eyelid skin that would have otherwise been discarded. This repair enabled replacement of the deep portion of the defect with similar thickness skin (flap) and the superficial portion of the defect with thin skin (graft) while keeping the lip position unchanged from the pre-operative appearance.