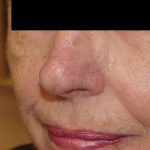
This patient was referred to Dr. Morganroth by one of his established patients after she heard about her wife’s friend’s long difficulty with a nostril basal cell carcinoma. The nostril basal cell carcinoma was initially diagnosed five years earlier and was treated with electrodessication and curettage followed by Aldara cream (imiquimod cream) by the patient’s general dermatologist. The tumor reappeared 6 months later and was treated again in the same manner. A few years later, the patient reported to his dermatologist that the nostril area would occasionally bleed. The area was treated with a deep shave and curettage. The patient presented over a year later to Dr. Morganroth with a fibrotic scar with a peripheral hemorrhagic crust (blood). A biopsy revealed infiltrative basal cell carcinoma with positive margins both deep and on the periphery of the biopsy. Mohs surgery was performed and after 4 Mohs layers, the pictured defect was observed.
This large defect presented a challenge due to its size and localization adjacent to the rim of the nostril. Due to the reconstruction challenges for a defect of this size and location, the most common reconstruction approach would likely be a full thickness skin graft harvested from the skin around the ear. While this creates an acceptable cosmetic result, the depth of this defect and proximity to the nostril rim presents a risk of the defect contracting and causing the nostril to move upward and flare. Distortions of the nose are particularly disturbing to patients and are impossible to conceal with make-up. Dr. Morganroth discussed the options of full thickness skin graft versus a paramedian forehead flap. The patient preferred the better tissue match and stability of the forehead flap but was not interested in a linear scar on his forehead and the three weeks of waiting with a pedicle trunk obstructing his vision until the second stage of the procedure. In an effort to provide the skin equivalent of the forehead flap but limit the cosmetic downtime of the forehead flap, Dr. Morganroth offered an innovative alternative of a two stage pedicle flap from the adjacent nasolabial fold where the post-op appearance could be hidden with a small bandage localized to the nostril. This pedicle flap would also require a smaller flap since the orientation of the defect was parallel to the nasolabial fold. In the case of a forehead flap, the widest dimension of the nasal defect would define the width of the superior aspect of the forehead flap and create a large defect requiring a flap repair of the forehead. The nasolabial pedicle flap would leave a linear scar hidden within the patient’s nasolabial fold — a significantly superior donor site outcome. The patient agreed with Dr. Morganroth’s suggestion and underwent a 20 minute local anesthesia procedure on the same days as his Mohs surgery. He returned 3 weeks later for the second stage of the repair which was a 10 minute procedure under local anesthesia. At a six month follow-up, high patient satisfaction was noted and an excellent result was observed without any recurrence of cancer.