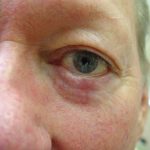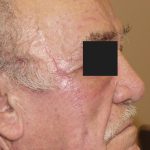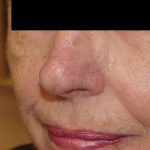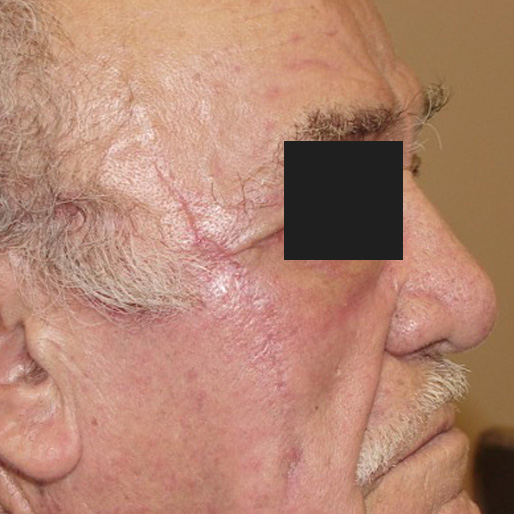
This patient sought Dr. Morganroth’s nationally-recognized expertise in Mohs surgery and facial reconstruction for a large, recurrent infiltrative basal cell carcinoma. The before photo shows a large temple, cheek and lateral canthus defect following Mohs surgery for a recurrent, infiltrative basal cell carcinoma treated by the patient’s dermatologist with excision and 5-fluorouracil cream. When the initial excision showed positive margins on the excision pathology report, the dermatologist attempted to treat the positive margin with topical chemotherapy cream without any success. Basal cell carcinomas on the face are best treated with Mohs surgery as the first line therapy for the highest cure rate and minimal sacrifice of normal tissue. Tumors with aggressive histologic features (infiltrative, morpheaform, basosquamous, perineurial) can be very destructive and have a lower cure rate with all other treatment options. This large defect was complicated because of the location adjacent to the eye and apparent lack of surrounding skin to recruit for a closure. Linear closure of this defect does not appear to be a possible option. The reconstruction options include granulation (allowing the defect to heal on its own), flap or adjacent tissue transfer, full thickness skin graft or a combination of these options. Dr. Morganroth has performed over 38,000 reconstructions and never plans a repair until wide undermining is performed. Wide undermining maximizes the mobility of the skin and often changes the reconstruction options. In this case, wide undermining allowed for an unexpected linear or primary closure of the defect. Any defect closed under high tension has a higher risk of dehiscence, infection, spitting stitches, scar hypertrophy and keloid and undesirable cosmetic result. In his unwavering goal to provide the best cosmetic and functional outcome, Dr. Morganroth closed the defect in a linear fashion up until the point the defect was under too much tension for a high likelihood of an excellent result. This approach left a central defect that was 90% smaller than the original defect. In order to complete 100% closure of the defect, a full thickness skin graft was utilized to fill the defect. Typically, full thickness skin grafts are harvested from the skin the skin around the ear, supraclavicular region, nasolabial folds or neck. In order to avoid creating an additional scar elsewhere, Dr. Morganroth recycled the excessive, non-hair bearing skin from superior temple resulting from the linear repair as the full thickness skin graft. This skin was removed to prevent a standing cone or “dog ear” of skin at the superior end of the linear repair that would have necessitated a revision procedure in the future. Normally, standing cone skin is discarded as medical waste, but in this case, Dr. Morganroth used this skin as a perfect match to the skin defect. It takes a year or more for reconstruction scars to fully mature. This one month post-operative photo looks very good but will continue to improve over the next year.