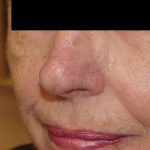
This patient had a very large nodular basal cell carcinoma on the tip of her nose for many years. Her children finally convinced her to see a dermatologist for treatment. Her dermatologist referred her to Dr. Morganroth, a double board certified Mohs surgeon who specializes in advanced reconstructive surgery under local anesthesia, for consideration of Mohs surgery for her very large tumor. Dr. Morganroth performed Mohs surgery over a number of hours to track out the tumor and preserve as much normal tissue as possible. Following Mohs surgery the resultant defect was extensive involving the entire nasal tip skin and cartilage, columella and cartilage, and upper lip and nasal exposing the septal cartilage located deep in the nose. The defect can also be understood anatomically if you grab the nasal tissue between the nostrils with your fingers and move the nasal skin around — all of the tissue you can move around was sacrificed. This nasal defect represented one of the most challenging reconstructions of Dr. Morganroth’s career and was complicated by the fact that the patient smoked two packs of cigarettes per day (smoking greatly increases the risk of failure of any reconstruction).
The surgery was planned immediately after the Mohs surgery was performed with local anesthesia alone. The reconstruction required the replacement of the nasal tip and columella cartilage and skin of the nasal tip, nasal columella, nasal sill and upper lip (skin from the base of the nostril extending to the upper lip). Using four cartilage grafts from the ear, the two nasal tip and two columella cartilages were reconstructed. A paramedian forehead flap was utilized to cover the cartilage grafts with forehead skin to restore a natural appearance to the distal nose. A bilateral rotation flap was utilized to reconstruct the upper lip and nasal sill. The paramedian forehead flap is a two-step pedicle procedure where the forehead skin is incised except for the inferior base of the flap at the medial eyebrow. This lower part of the flap remains attached to the medial eyebrow as the forehead skin flap is rotated and attached to the distal nose. The flap receives its blood supply from the medial eyebrow artery via the trunk of tissue to nourish the forehead skin that is now attached to the distal nose similar to an umbilical cord. After three weeks, the forehead skin that was sewn over the cartilage grafts develops its own blood supply from the surrounding tissue of the nasal tip and the pedicle/umbilical cord is no longer needed. The forehead flap pedicle is divided and the excess skin is discarded. The final repair seen three months after surgery created a remarkable restoration. Patients interested in seeing a pictorial of the entire procedure from start to finish may view the photos at our office.