This patient underwent Mohs surgery by another Mohs surgeon in the SF Bay Area who declined to perform a reconstruction. The patient was discharged without a treatment plan and sought reconstruction options on his own. He was seen at the plastic surgery department of an academic center who recommended a paramedianl forehead flap which is a multi-stage reconstruction procedure with multiple surgeries performed over a three week period under general anesthesia. The patient was not comfortable with an extensive 3 hour procedure under general anesthesia and continued his search for an experienced reconstructive surgeon with an innovative approach. The patient self-referred to Dr. Morganroth based on his own research. On presentation to Dr. Morganroth, the patient had a partially healed nasal defect due to the two week delay in finding a reconstructive surgeon. With many thousands of nasal reconstructions over his career, Dr. Morganroth agreed with the plastic surgeon that a paramedian forehead flap was a good option due to the very large size of the defect. Dr. Morganroth explained that he could perform the forehead flap in less than 30 minutes with local anesthesia and the second procedure would take place three weeks later and take less than 15 minutes under local anesthesia. Despite the shorter operative time and local anesthesia, the patient did not want to have his forehead attached to his nose for three weeks and then have more recovery after the required second surgery.
Dr. Morganroth discussed a flap or full thickness skin graft as potentially inferior alternatives to the multi-step paramedian forehead flap surgery recommended by the academic center. After discussing the positives and negatives of flaps versus full thickness skin grafts, the patient selected the flap option for the best skin texture, color and thickness match for the missing nasal tip skin. Since the skin defect had been healing for two weeks while looking for a surgeon to repair the defect, the skin defect margin had been healing and now had to be excised to create fresh skin edges prior to the flap reconstruction to ensure proper healing.
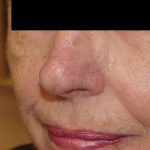
Dr. Morganroth repaired this defect with a bilobed transposition flap that extended up to the glabella (skin between the eyebrows) completely under local anesthesia in 20 minutes. In simple terms, the loose skin of the glabella was moved to the bridge of the nose and the skin of the bridge of the nose (which was the best match for the missing skin) was moved into the nasal tip defect. Flaps move skin from areas of loose skin to areas of high tension. Dr. Morganroth’s flap provided an outcome with many advantages over a forehead flap including the use of better matched nasal skin to fill the defect, the avoidance of a large forehead scar from a forehead flap, and the avoidance of multiple general anesthesia procedures.